The Coronary Atlas
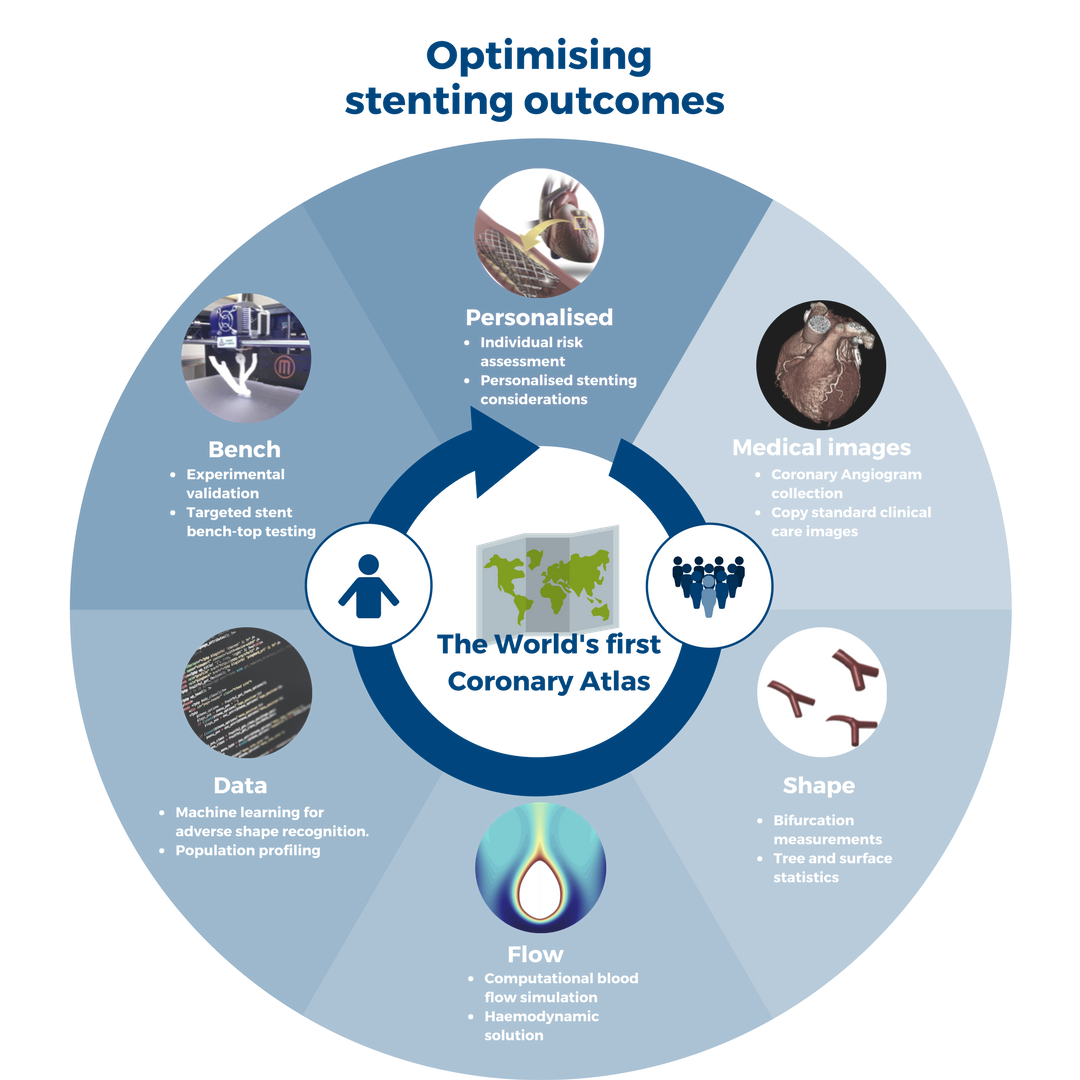
The coronary atlas project aims to understand individual differences in the blood flow environment to generate insights into disease susceptibility for prevention and treatment improvement.
For heart disease patients worldwide
Describing the detailed statistical anatomy of the coronary artery tree is important for determining the ætiology of heart disease. A number of studies have investigated geometrical features and have found that these correlate with clinical outcomes, e.g. bifurcation angle with major adverse cardiac events.
These methodologies were mainly two-dimensional, manual and prone to inter-observer variability, and the data commonly relates to cases already with pathology.
In contrast, the Coronary Atlas uses hybrid atlasing methodology to build a population of computational models of the coronary arteries to comprehensively and accurately assess anatomy including 3D size, geometry and shape descriptors.
A random sample of more than 1200 cardiac 64-CT 3D scans with a calcium score of zero was segmented and analysed using a standardised protocol. The resulting atlas includes, but is not limited to, the distributions of the coronary tree in terms of angles, diameters, centrelines, principal component shape analysis and cross-sectional contours.
This novel resource will facilitate the improvement of stent design and provide a reference for hemodynamic simulations, and provides a basis for large normal and pathological databases.
Global context
Global mortality rate
- Coronary artery disease
- Stroke
- Dementia
- Diabetes
- Cancer
A coronary event happens every…
The cost of coronary disease USD
Publications
Combining medical and engineering sciences
Construction of a coronary atlas from CT angiography
Medrano-Gracia, P., et al. Construction of a coronary atlas from CT angiography. in Medical Image Computing and Computer Assisted Intervention. 2014. Boston, USA.
Describing the detailed statistical anatomy of the coronary artery tree is important for determining the ætiology of heart disease. A number of studies have investigated geometrical features and have found that these correlate with clinical outcomes, e.g. bifurcation angle with major adverse cardiac events.
These methodologies were mainly two-dimensional, manual and prone to inter-observer variability, and the data commonly relates to cases already with pathology. We propose a hybrid atlasing methodology to build a population of computational models of the coronary arteries to comprehensively and accurately assess anatomy including 3D size, geometry and shape descriptors.
A random sample of 122 cardiac CT scans with a calcium score of zero was segmented and analysed using a standardised protocol. The resulting atlas includes, but is not limited to, the distributions of the coronary tree in terms of angles, diameters, centrelines, principal component shape analysis and cross-sectional contours. This novel resource will facilitate the improvement of stent design and provide a reference for hemodynamic simulations, and provides a basis for large normal and pathological databases.
A Study of Coronary Bifurcation Shape in a Normal Population
Medrano-Gracia, P., et al., A Study of Coronary Bifurcation Shape in a Normal Population. Journal of Cardiovascular Translational Research, 2016: p. 1-9.
Abstract
During percutaneous coronary intervention, stents are placed in narrowings of the arteries to restore normal blood flow. Despite improvements in stent design, deployment techniques and drug-eluting coatings, restenosis and stent thrombosis remain a significant problem.
Population stent design based on statistical shape analysis may improve clinical outcomes. Computed tomographic (CT) coronary angiography scans from 211 patients with a zero calcium score, no stenoses and no intermediate artery, were used to create statistical shape models of 446 major coronary artery bifurcations (left main, first diagonal and obtuse marginal and right coronary crux). Coherent point drift was used for registration.
Principal component analysis shape scores were tested against clinical risk factors, quantifying the importance of recognised shape features in intervention including size, angles and curvature. Significant differences were found in (1) vessel size and bifurcation angle between the left main and other bifurcations; (2) inlet and curvature angle between the right coronary crux and other bifurcations; and (3) size and bifurcation angle by sex.
Hypertension, smoking history and diabetes did not appear to have an association with shape. Physiological diameter laws were compared, with the Huo-Kassab model having the best fit. Bifurcation coronary anatomy can be partitioned into clinically meaningful modes of variation showing significant shape differences.
A computational atlas of normal coronary bifurcation shape, where disease is common, may aid in the design of new stents and deployment techniques, by providing data for bench-top testing and computational modelling of blood flow and vessel wall mechanics.
A Computational Atlas of Normal Coronary Artery Anatomy
Medrano-Gracia, P., et al., A Computational Atlas of Normal Coronary Artery Anatomy. EuroIntervention, 2016. EIJ-D- 16-00111(in press).
Aims
The aim of this study was to define the shape variations, including diameters and angles, of the major coronary artery bifurcations.
Method and results
Computed tomographic angiograms from 300 adults with a zero calcium score and no stenoses were segmented for centreline and luminal models. A computational atlas was constructed enabling automatic quantification of 3D angles, diameters and lengths of the coronary tree. The diameter (mean±SD) of the left main coronary was 3.5±0.8 mm and the length 10.5±5.3 mm. The left main bifurcation angle (distal angle or angle B) was 89±21° for cases with, and 75±23° for those without an intermediate artery (p<0.001). Analogous measurements of diameter and angle were tabulated for the other major bifurcations (left anterior descending/diagonal, circumflex/obtuse marginal and right coronary crux). Novel 3D angle definitions are proposed and analysed.
Conclusions
A computational atlas of normal coronary artery anatomy provides distributions of diameter, lengths and bifurcation angles as well as more complex shape analysis. These data define normal anatomical variation, facilitating stent design, selection and optimal treatment strategy. These population models are necessary for accurate computational flow dynamics, can be 3D printed for bench testing bifurcation stents and deployment strategies, and can aid in the discussion of different approaches to the treatment of coronary bifurcations.
Impact of bifurcation angle and other anatomical characteristics on blood flow–A computational study of non-stented and stented coronary arteries.
Beier, S., et al., Impact of bifurcation angle and other anatomical characteristics on blood flow–A computational study of non-stented and stented coronary arteries. Journal of biomechanics, 2016. 49(9): p. 1570-1582.
Abstract
The hemodynamic influence of vessel shape such as bifurcation angle is not fully understood with clinical and quantitative observations being equivocal. The aim of this study is to use computational modeling to study the hemodynamic effect of shape characteristics, in particular bifurcation angle (BA), for non-stented and stented coronary arteries. Nine bifurcations with angles of 40°, 60° and 80°, representative of ±1 SD of 101 asymptomatic computed tomography angiogram cases (average age 54±8 years; 57 females), were generated for (1) a non-stented idealized, (2) stented idealized, and (3) non-stented patient-specific geometry.
Only the bifurcation angle was changed while the geometries were constant to eliminate flow effects induced by other vessel shape characteristics. The commercially available Biomatrix stent was used as a template and virtually inserted into each branch, simulating the T-stenting technique. Three patient-specific geometries with additional shape variation and ±2 SD BA variation (33°, 42° and 117°) were also computed.
Computational fluid dynamics (CFD) analysis was performed for all 12 geometries to simulate physiological conditions, enabling the quantification of the hemodynamic stress distributions, including a threshold analysis of adversely low and high wall shear stress (WSS), low time-averaged WSS (TAWSS), high spatial WSS gradient (WSSG) and high Oscillatory Shear Index (OSI) area.
The bifurcation angle had a minor impact on the areas of adverse hemodynamics in the idealized non-stented geometries, which fully disappeared once stented and was not apparent for patient geometries. High WSS regions were located close to the carina around peak-flow, and WSSG increased significantly after stenting for the idealized bifurcations.
Additional shape variations affected the hemodynamic profiles, suggesting that BA alone has little effect on a patient׳s hemodynamic profile. Incoming flow angle, diameter and tortuosity appear to have stronger effects. This suggests that other bifurcation shape characteristics and stent placement/strategy may be more important than bifurcation angle in atherosclerotic disease development, progression, and stent outcome.
Research
{kind=link}
Your role
The Coronary Atlas project welcomes collaboration and involvement by interested parties. If you are a researcher, cardiologist, developer or student with a professional interest in the project, please get in touch.

Patients
Want to know more about our research? Look at the Global context page, or listen to the RadioNZ interview of the atlas
Cardiologists
Want to contribute? Contact the team. Keep updated with the latest interventional strategy recommendations see our talks.

Researchers
Do you want to contribute or us to share CTCA images, STL files for computing or 3D printing? Or access to the statistical data? No problem. Contact us for details.

Developers
Want to explore, have ideas or want to create your own? We are happy to chat. Contact us for details.

Students
We are currently recruiting Masters and Ph.D. students and are happy to accept interns. Contact us for more information.
Funding
So far the Coronary Atlas has attracted over $2,100,000 in funding
Global mortality rate
Sponsors





Collaborators


